INVITAE · SERVICE DESIGN · AI/ML · OPERATIONAL TOOLS
Designing the Human Layer in an Automated System

The challenge
Invitae's mission was to bring comprehensive genetic information into mainstream medicine making testing affordable and accessible to everyone. The organization was doing exactly that, often processing genetic tests regardless of whether insurance would pay for them.
The result was a growing gap between tests delivered and revenue collected. The Orders to Cash initiative was a company-wide strategic effort to close that gap. Not by turning patients away, but by building smarter, more automated systems that could handle the volume without breaking.
Three projects, one mission
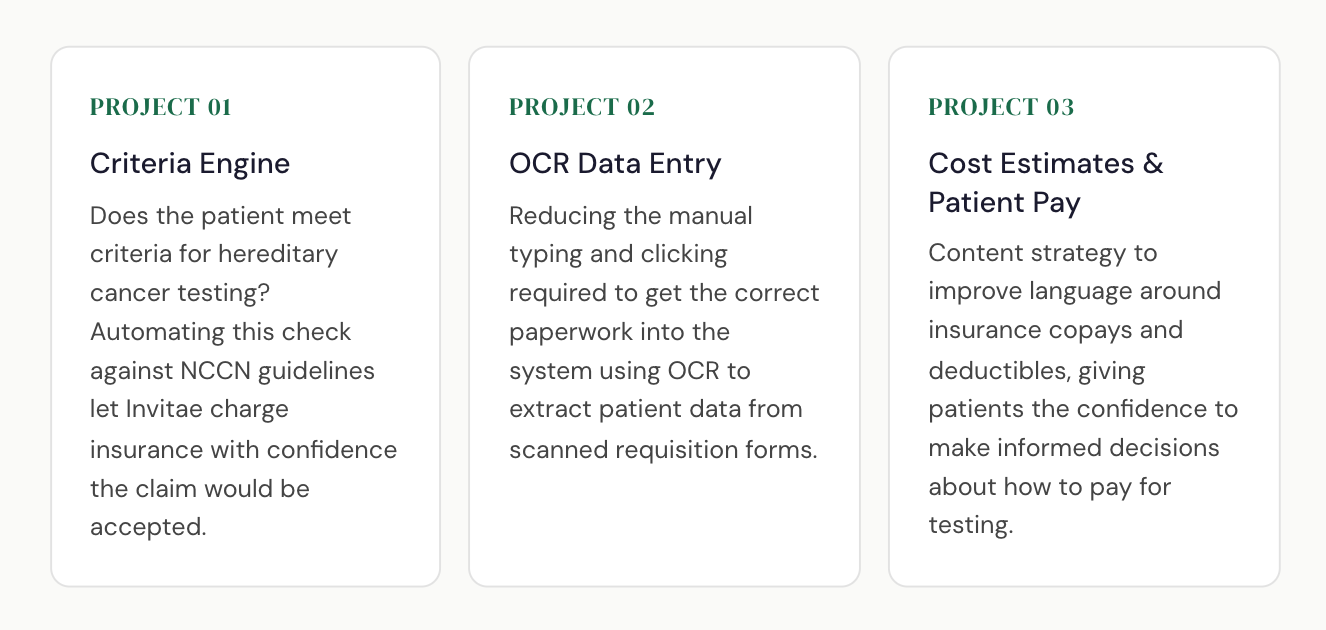
Orders to Cash was a portfolio of three interconnected initiatives, each targeting a different part of the order lifecycle:
The gap design was brought in to fill
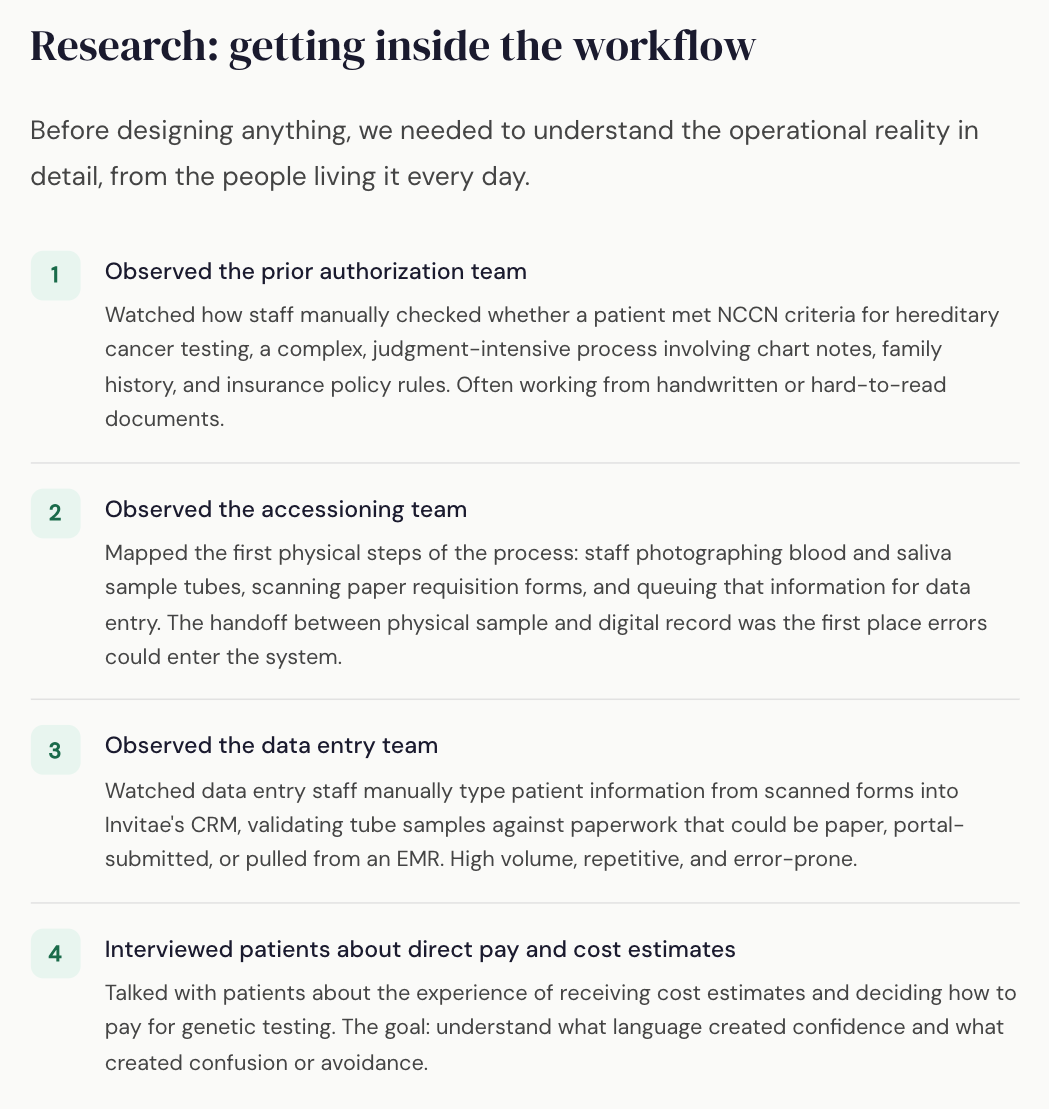
The Orders to Cash initiative had just started before joining the team. What became obvious within the first discussions, there was a need for service design to anchor this work. The engineering and ML teams were building, but they were building blind. They had never observed the people who would use what they were creating. There was no shared picture of how an order actually moved through the organization from intake to reimbursement.
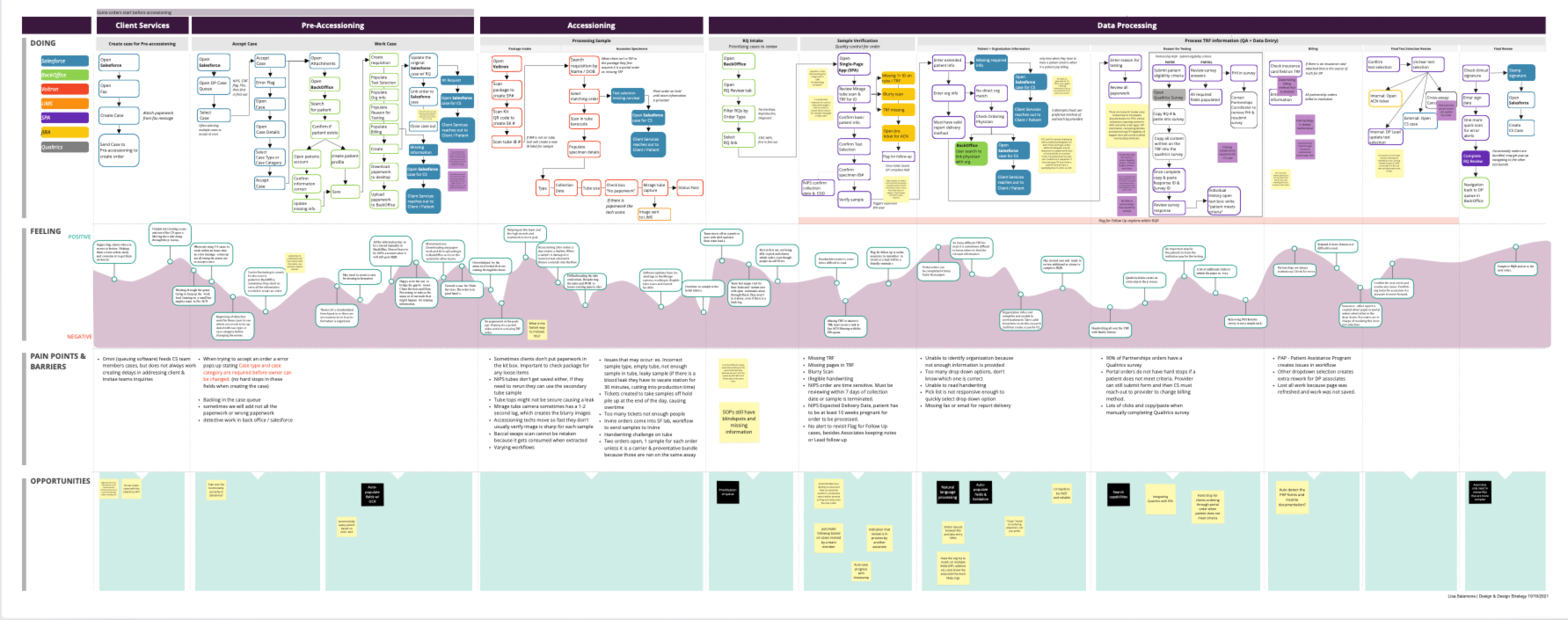
The "life of the order" workshop
After research, we facilitated a workshop with engineers, product managers, the UX designer, and the VP of ML. We walked the entire team through a full map of how an order moved through the organization, every step, every handoff, every person and demoed the actual operational experience they were building for.
For many in the room, it was the first time they had seen the full picture. The complexity of what the operations teams were managing manually and the human effort behind what the ML was supposed to replace landed differently when it was visible all at once.
That was the first thing we needed to fix.
What we designed
Project 01: Criteria Engine: the medical necessity review interface
The ML model automated approximately 60–66% of order volume cases where the patient clearly met NCCN criteria. The remaining 40% required a human reviewer. We designed the interface for that human layer.
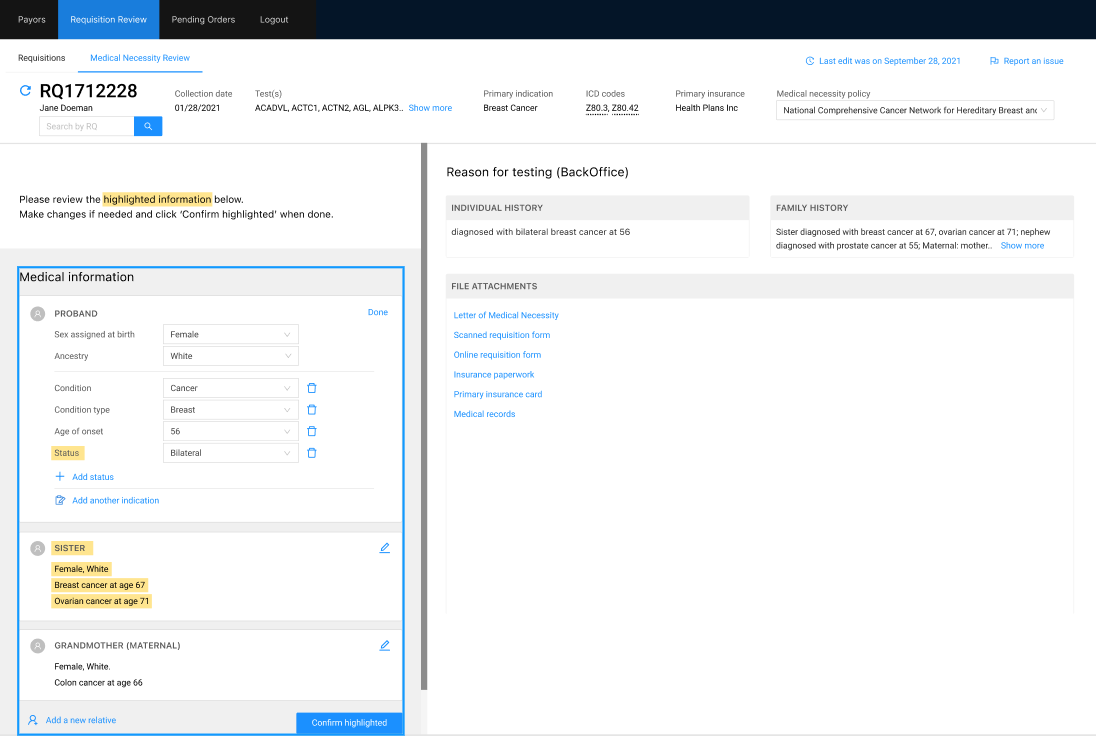
Key design decisions in this interface:
Highlighting what the system wasn't sure about
The ML algorithm had flagged yellow highlights on fields with low confidence scores. Reviewers could see exactly why the case wasn't auto-accepted and what needed human judgment.
Designing the final sign-off as a deliberate action
"Confirm highlighted" was the single point of accountability .
Keeping the source document in view
Chart notes and requisition forms were often handwritten and hard to read. The right panel kept the original document visible alongside the structured form.
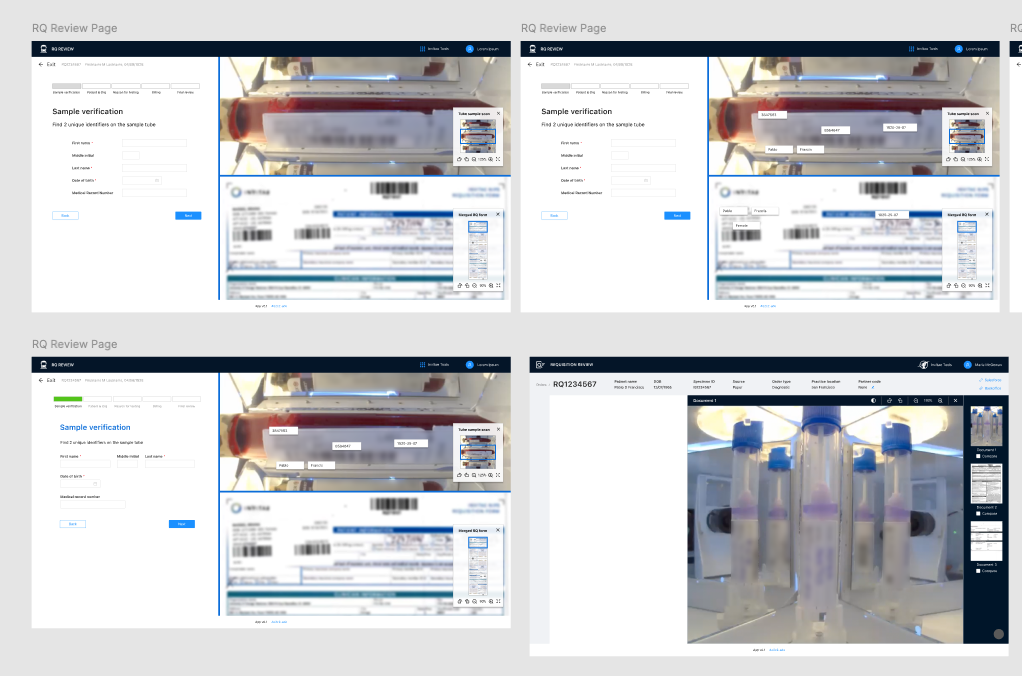
Project 02: OCR Data Entry: the document extraction interface
The OCR tool extracted patient information from scanned paper requisition forms and pre-populated the CRM entry form. Data entry staff reviewed, corrected, and confirmed what the system had pulled with a split-screen experience where the source document panel could be opened, closed, or swapped for other documents as needed.
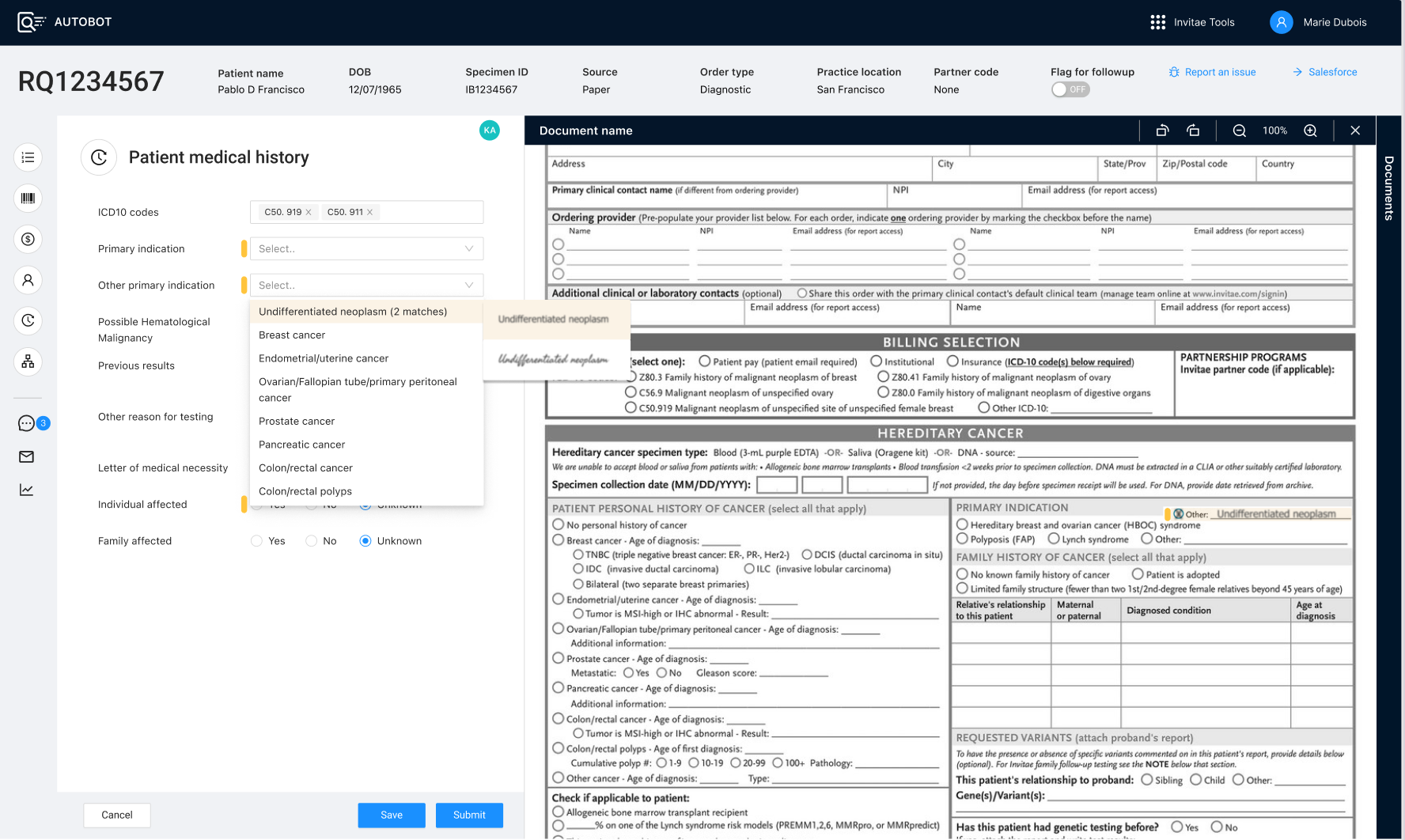
Key design decisions in this interface:
Orange indicators signal required human confirmation
Fields flagged with orange weren't necessarily wrong — they were fields where the system needed a deliberate human sign-off before the record could be submitted. This distinction mattered: it shifted the interaction from "fix the error" to "confirm the decision.
A collapsible, swappable document panel
The scanned requisition was shown by default on the right side of the screen, but staff could collapse it or pull up other source documents, insurance paperwork, EMR records, portal submissions depending on what they needed to cross-reference.
Structured selection over free-text: to train the model
When the OCR got something wrong, the first corrective path was a structured dropdown or selection list rather than a free-text field. This was a deliberate design decision: structured corrections could be fed back into the ML model to improve future extractions.
The hardest design challenge: trust and behavior change
The ML model was still learning when the tools launched. It made mistakes and operations staff noticed. The most common piece of feedback during early testing: "It would just be easier for me to do this myself."
This wasn't resistance to technology. It was a reasonable response to a system that wasn't yet reliable enough to justify the cognitive overhead of reviewing its errors. But there was a deeper challenge underneath it: to improve, the model needed staff to correct it in a structured way, through selection lists rather than free-text typing. That meant asking people to change a deeply ingrained behavior in exchange for a benefit they couldn't yet see.
Impact
66–76% of orders meeting criteria automated end-to-end with no human review required
Prior auth and billing staff freed from routine cases to focus on complex ones that genuinely required clinical judgment
Staff corrections to OCR and criteria outputs used to improve ML model accuracy over time
"Life of the order" workshop created shared organizational understanding that drove prioritization across the two internal projects
OCR data entry tool in final deployment phases at time of departure; criteria engine and cost estimate work fully launched
Patient-facing cost estimate language redesigned to improve confidence and reduce avoidance around insurance copay decisions